Important Notice
If you are a doctor, dietitian, nurse, pharmacist, then click on I’m a healthcare professional to proceed. For persons other than Health care professionals, we request you to visit www.danone.in.
A 3-month-old unwell baby girl presented with vomiting, lethargy, and oliguria to a Paediatric Gastroenterologist and was admitted in the hospital.
The baby was born full term and healthy at birth, weighing 3.8 kgs (weight/age z score = 0 to -2) to non-consanguineous parents. 21 days after birth, she developed persistent vomiting and diarrhea for which she was treated with antibiotics. This reduced her stool frequency, but the symptoms persisted. Her weight gain was very poor. At 6 weeks, she weighed about 3.7 kgs and continued to pass stool at an increased frequency.
Apart from breastfeeding, the baby was top fed and made to change 2 different cow’s milk formulas and then was kept on soy formula. At 3 months of age, she was very unwell and had to be brought to the hospital.
On primary examination at the time of admission, the baby appeared to be lethargic and oliguric due to persistent vomiting, severe dehydration, tachycardia and tachypneia. She weighed 3.4 kgs (weight/age z score = < -3 = severely underweight). We admitted her in the Neonatal Intensive Care Unit and she was resuscitated, rehydrated and stabilized.
Laboratory examination upon admission showed:
Venous Blood gasses
Endoscopy revealed a complete non-development of the villous (Refer Figure 1). We excluded metabolic disorders and structural intestinal problems.
Chronic vomiting, diarrhea, dehydration, lethargy and weight loss are indicative of Food Protein-Induced Enterocolitis Syndrome (FPIES). Based on the clinical presentation, she was a suspect of FPIES. At first, intravenous fluid resuscitation was done. We eliminated cow’s milk and soy protein from her diet and on day 2 started with amino acid-based infant formula which was well tolerated by her. A reduction in diarrhea was observed from the 4th day and by the 8th day the patient was stable enough to be discharged from the hospital.
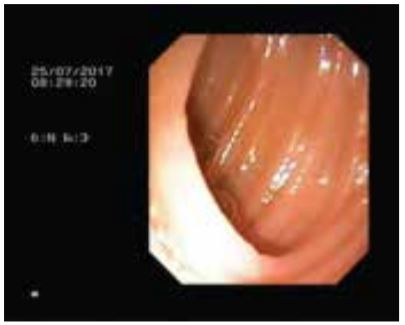 Endoscopy revealed a complete non-development of the villous.
Endoscopy revealed a complete non-development of the villous.
Birth to 6 months (z-scores)
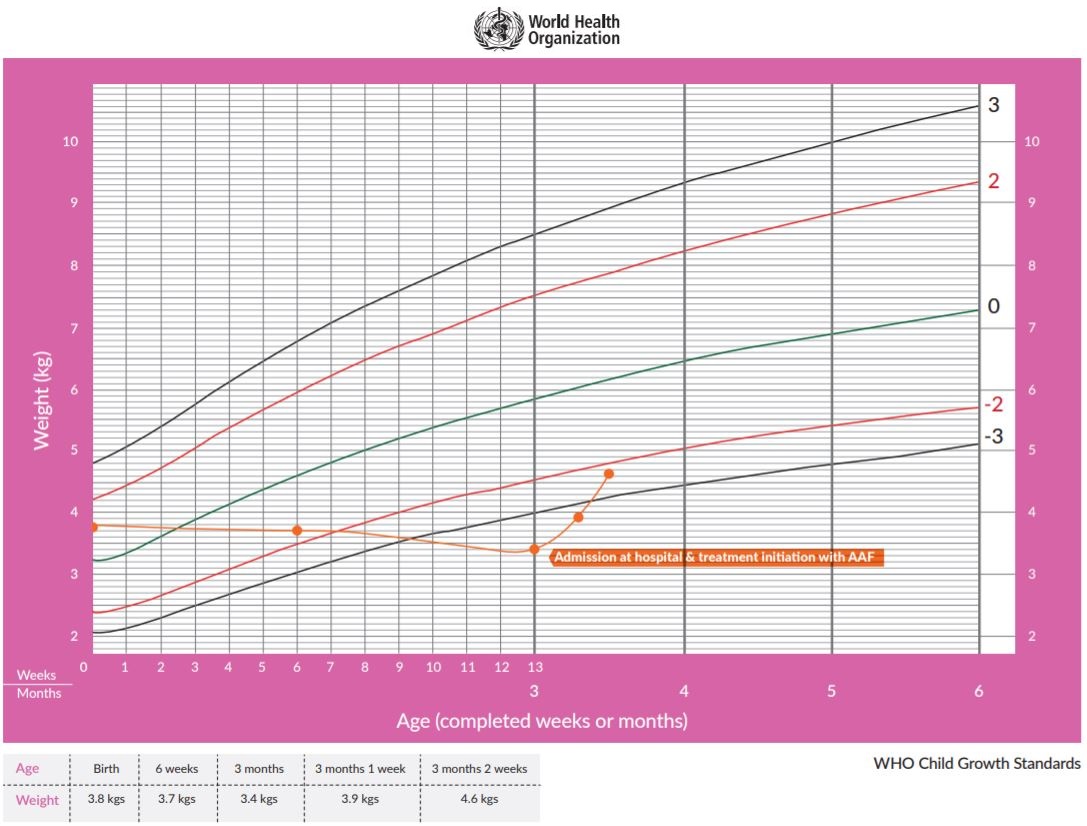 WHO Child Growth Standards chart sourced from http://www.who.int/childgrowth/standards/cht_wfa_girls_z_0_6.pdf?ua=1. Accessed on 16.08.2018
WHO Child Growth Standards chart sourced from http://www.who.int/childgrowth/standards/cht_wfa_girls_z_0_6.pdf?ua=1. Accessed on 16.08.2018
Her weight at the time of discharge was 3.9 kgs. The patient remained symptom-free in the following days and reported back to the outpatient department 7 days later. With treatment on AAF (Amino acid formula), she showed substantial weight gain and was now at 4.6 kgs (weight/age z score = -2 to -3) climbing on the growth curve (Refer Figure 2).
Food protein-induced enterocolitis syndrome (FPIES) is considered the most severe of the non-IgE-mediated gastrointestinal (GI) food allergies that typically presents in infancy. Onset can occur within 1–4 hours after the ingestion of the offending foods and children typically are negative to food specific IgEs.1
It has been hypothesized that ingestion of food allergens causes local inflammation leading to increased intestinal permeability and fluid shift, which results in the symptoms of vomiting, diarrhea and lethargy which are all characteristic of FPIES.2 Severe cases can progress to hypothermia, methemoglobinemia, acidemia, and hypotension, mimicking sepsis.1
FPIES does not occur in breastfed infants and seems to require direct ingestion of the allergen by infant.3 Cow’s milk, soy and grains are commonly reported triggers of FPIES.1 In the present case, the baby was allergic to cow’s milk and soy protein and its elimination led to symptom improvement.
Symptoms of FPIES overlap with other medical conditions, so diagnosis can be challenging.
The diagnosis is based on medical history and absence of symptoms when the causative food is eliminated from the diet. FPIES food challenge generally is not performed before 2 yrs of age.3
Management of FPIES includes elimination of food allergen, guidance on foods that can be consumed and continuous assessment of nutritional intake as well as growth and development. The present case was a chronic FPIES with symptoms including vomiting, chronic diarrhea and failure to thrive. Typically infants with chronic FPIES usually return to their usual state of health within 3-10 days of switching to a hypoallergenic formula.1 European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) guidelines recommend the use of AAF for the treatment of FPIES, particularly in association with growth faltering.4
After treatment with AAF, we observed considerable improvement in her weight. The decision to choose an AAF over an eHF was because eHF contains residual peptides and may not give complete symptom resolution. The choice of formula can be made on the basis of the clinical presentation but studies have shown that eHF may not be suitable for treatment of FPIES in all infants.5,6
Delay and misdiagnosis of FPIES is common and this entity needs to be understood well. The present case illustrates the importance of appropriate nutritional management with an AAF in FPIES to ensure normal growth and development.
References:-
Nowak-Wegrzyn A. et al. International consensus guidelines for the diagnosis and management of food protein–induced enterocolitis syndrome: Executive summary—Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J allergy clin immunol april 2017.
Caubet J, Nowak-Wegrzyn A. Current understanding of the immune mechanisms of food protein-induced enterocolitis syndrome. Expert Rev Clin Immunol 2011;7:317–327.
Koletzko B et al. Pedaitric Nutrition in Practice. 2nd revised edition, Karger. World review of Nutrition and dietetics, Vol 113.
Koletzko S, Niggemann B, Arato A, et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: Espghan GI committee practical guidelines. J Pediatr Gastroenterol Nutr. 2012;55(2):221-229.
Vanderhoof JA et al. Intolerance to protein hydrolysate infant formulas: an underrecognized cause of gastrointestinal symptoms in infants. J Pediatrics 1997;131:741–774.
Kelso JM, Sampson HA. Food protein-induced enterocolitis to casein hydrolysate formulas. J Allergy Clin Immunol 1993; 92:909–910.
Important Notice:
The World Health Organization (WHO)* has recommended that pregnant women and new mothers be informed of the benefits and superiority of breast-feeding, in particular, the fact that it provides the best nutrition and protection from illness for babies. Mothers should be given guidance on the preparation for and maintenance of lactation, with special emphasis on the importance of the well-balanced diet both during pregnancy and after delivery. Unnecessary introduction of partial bottle feeding or other foods and drinks should be discouraged since it will have a negative effect on breast-feeding. Similarly mothers should be warned of the difficulty of reversing a decision not to breastfeed. Before advising a mother to use an infant formula, she should be advised of the social and financial implications of her decision. For example, if a baby is exclusively bottle-fed, more than one can (500g) per week will be needed, so the family circumstances and cost should be kept in mind. Mother should be reminded that breast milk is not only the best but also the most economical food for babies. If a decision to use infant formula is taken, it is important to give instruction on correct preparation methods, emphasizing that unboiled water, unsterilized bottles or incorrect dilution can lead to illness.
*See: International Code of Marketing of Breast Milk Substitutes, adopted by the World Health Assembly in Resolution WHA 34.22, May 1981.
Mothers should be explained the following advantages & nutritional superiority of breastfeeding:
Details of management of breast feeding, as under:
